48uep6bbphidvals|334
48uep6bbph|2000F98CTab_Articles|Fulltext
The human esophagus is a 25 to 35 cm long muscular tube.[1] The contractions of the esophagus propel food into the stomach and also help to clear refluxed acid back to the stomach. The lower esophageal sphincter (LES) remains tonically contracted preventing reflux of acid from stomach to the esophagus. LES relaxes during swallowing, vomiting and belching to allow foods and gastric contents to pass into and out of the stomach. Tests of esophageal function evaluate contraction of its muscle and the movement of the food bolus and refluxate resulting from it. It also evaluates exposure of the esophagus to acid. These tests include (a) contrast radiography, (b) manometry, (c) 24-h ambulatory pH-metry and impedance monitoring, (d) radionuclide esophageal transit studies. The latter three methods will be reviewed in this article.
Esophageal manometry equipment
Esophageal manometry is performed either with water perfusion or with solid state system.[2] The solid state system, though more sensitive to pressure changes, is expensive and fragile. Therefore, water perfusion system is preferred in most centers. Water perfusion system consists of several capillary tubes connected to a multilumen perfusion catheter (usually 6-8 lumen) and external transducers. These tubes are continuously perfused with deaerated water at a constant rate (approximately 0.5 ml/min) by a low compliance pneumohydraulic pump powered by compressed nitrogen.[3] Each lumen of the catheter terminates in a side hole and senses intraluminal pressure of esophagus by relative obstruction to flow of perfused water. Currently, we are using a water perfusion system with a catheter having 8 side-holes. The proximal four side holes, which are 5 cm apart, are positioned in the esophageal body while the distal four, placed circumferentially, are in the lower esophageal sphincter (LES) zone. Intra-gastric pressure is used as baseline for any pressure measurement. Each capillary tube, opening at a side-hole at one end is connected to an external transducer at the other end in such a way that the tracing from the most proximal port is displayed at the top of the computer screen and that from the most distal port appears at its bottom. Esophageal manometery records contractions of circular muscles and not that of longitudinal muscles.
Technique
Patient preparation: Esophageal manometry is performed after overnight fast. All the drugs that may interfere with esophageal motility and LES pressure (prokinetics, calcium channel blockers, anticholinergics etc.) should be discontinued at least 48-h prior to the study. Patients are not sedated, as their cooperation is essential for the study. The procedure is explained to the patient.
Intubation and placement of the catheter: Manometry catheter is passed through one nostril into the stomach. An extra length of the catheter is initially inserted so as to have all the 8 ports inside the stomach. The location of catheter ports can be confirmed by noting the effect of inspiration on pressure tracing or by noting a rise in pressure in all ports by pressure over the epigastrium. Inspiration causes an upward deflection in pressure recording if the opening of the catheter is in the stomach whereas a downward deflection is produced if the same is in the esophagus.
Study of LES pressure: LES pressure can be assessed either by station pull-through (SPT) or by rapid pull-through (RPT) techniques.[3] During SPT, the manometry catheter is gently and gradually pulled out, through a small length (1-cm) at a time, and pressure is recorded at each site. Each port reaches a point where it shows a rise in pressure that passes through the highpressure zone and, finally, reaches a point where pressure becomes low again. The length of high-pressure zone is determined taking the mean of values obtained from each port. When the manometry catheter port is in LES, inspiration causes an exaggerated rise in pressure; when the port crosses LES and lies in esophageal body, inspiration causes lowering of pressure tracing due to negative intrathoracic pressure generated during inspiration. This point where pressure tracing changes is known as pressure inversion point or point of respiratory reversal.[3]
Study of body motility: We study esophageal body motility with 4 distal circumferential ports at LES and 4 proximal ports at esophageal body. Body motility may be studied in response to dry and wet swallows. However, non-specific abnormalities in body motility in response to dry swallows may be found even in normal subjects. Therefore, we study body motility and LES relaxation in response to 10 wet swallows. For study of body motility, patient is instructed to swallow only on command. 5-ml water is given in each swallow. One must wait for 30 seconds between two swallows to avoid the phenomenon of deglutitive inhibition.[4] The timing of the swallow is marked on the screen using appropriate keyboard command to allow subsequent analysis of the record.
Study of LES pressure by rapid pull through: On completion of SPT, the catheter is pushed back into stomach again. After waiting for 1-2 minutes, the patient is asked to hold his breath in quiet expiration and refrain from swallowing. The catheter is then gently but steadily pulled out across LES.
Interpretation
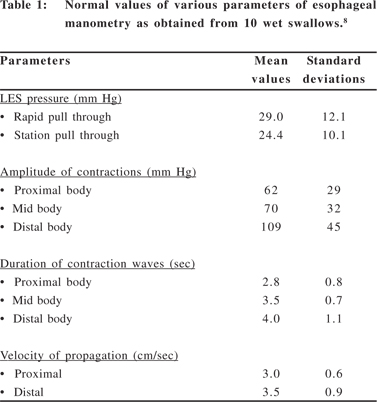
Currently, most laboratories use computer-based programs for acquisition and analysis of the recorded data. The parameters analyzed include, (a) LES parameters (resting pressure, length of the high pressure zone, relaxation in response to wet swallows and three-dimensional pressure profile), (b) body motility (amplitude, duration and abnormalities of each contraction wave e.g. double or multiple peaks, whether spontaneous contractions are present, whether contraction are propagated or simultaneous and if propagated, velocity of propagation).[5] We prefer using SPT technique for assessment of most of the above parameters of LES function.[6] The average value of several measurements from different ports obtained in mid-expiratory phase is taken as basal LES pressure. RPT has several disadvantages.[5] It may show spuriously low LES pressure if the patient took an inadvertent dry swallow at the time of RPT. LES relaxation is determined as the minimum pressure observed during a swallow. Relaxation should be considered normal if LES pressure drops greater than 90% from mean resting LES pressure.[7]Normal values of different parameters of esophageal manometry and criteria for diagnosis of various esophageal motility disorders are given in Table 1 and Table 2, respectively.[8, 9] Figure 1 shows manometry tracings in various motility disorders. Studies describing normal values of esophageal manometry in Indians are awaited.

Clinical utility
Esophageal manometry is useful in diagnosis of several diseases like achalasia cardia, diffuse esophageal spasm and nutcracker esophagus .[9,10,11,12] In fact, manometry is the gold standard for the diagnosis of these conditions. Manometry may also be useful in evaluating the effect of treatment in achalasia cardia.[13] In some diseases like gastroesophageal reflux disease (GERD), manometry may be useful in prognosis. Several studies showed that patients with GERD and very low LES pressure (<10 mm Hg) often have severe disease.[14] Some studies suggested partial fundoplication in patients with GERD and low amplitude contractions (<30 mm Hg) in distal esophagus,[15] though this has been debated.[16] In systemic diseases such as progressive systemic sclerosis, involvement of esophagus as diagnosed by manometry[17] and may be associated with severe GERD and reduced quality of life. Patients treated with endoscopic sclerotherapy for esophageal varices in the past, may have non-specific changes in esophageal manometry[18] that should be remembered while interpreting manometry tracing.
High Resolution Manometry (HRM)
HRM is a relatively new technology, foundation of which was laid in the early 1990s by Clouse and Staiano. Pressure profile was assessed during several swallows using catheter having multiple ports at closely spaced positions in the oesophagus. Time, catheter position and average pressure were then reconstructed into pseudo-3D ‘‘topographic plots’’ that demonstrated the functional anatomy of the oesophagus and that of the gastro-oesophageal junction. There are several advantages of HRM over conventional manometry most important of which are ease of performance and better ability to diagnose and classify esophageal motility disorders.
Equipment
Most of the HRM systems use solid state instead of water perfusion catheters. However, we use water perfusion catheter in our HRM system as solid state catheters are costlier. The number of ports in catheters of HRM may vary from 16 to 64. We use a catheter with 16 ports, of which upper 8 ports (3 cm apart) record body motility and lower 8 (1 cm apart) evaluate LES.
Technique
Patient preparation and catheter introduction for HRM are same as in conventional manometry.
Study of the body motility and LES: In contrast to conventional manometry, SPT need not be done to assess LES during HRM as location of LES is seen through isobaric pressure in colored scale. This reduces patient’s discomfort. As in conventional manometry, esophageal body motility is evaluated by 10 or more water swallows (5 ml each) every 30 sec. It is displayed in time, duration and pressure either through color plot, contour plot, line tracing or 3-dimensional plot.
Interpretation
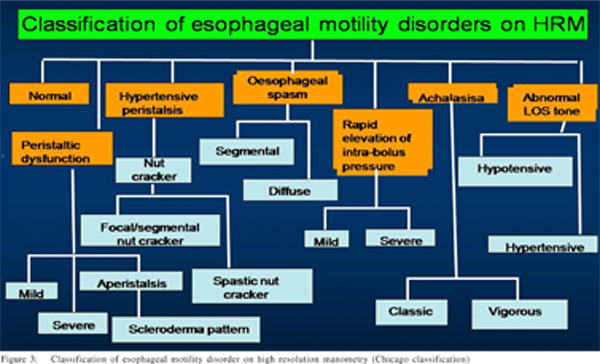
Appearance of HRM signals is appreciable easily due to color plots. In addition to normal features, one can pick up the segmental nature of the esophageal peristalsis, abnormal bolus transport due to poor contraction, long transition zone and focal spasm in the mid esophagus.[19,20] Figure 2 shows tracings of HRM in various esophageal motility disorders recorded in our laboratory. It is very useful to differentiate vigorous achalasia, diffuse esophageal spasm (DES) and prolonged or repetitive nutcracker which may be difficult sometimes in conventional manometry.[21] Hiatus hernia may also be seen in patients with GERD in HRM by movement and interaction of intrinsic LES and diaphragm.[22,23] Using conventional manometry, esophageal motor disorders can be classified into five groups (Table 2). Due to advanced technique of HRM the diagnostic criteria for esophageal motility disorders has been improved and classification into several sub-groups has been possible (Figure 3).[24]
Clinical utility
In conventional manometry, abnormal motility patterns present in a short segment of the esophagus, may be missed. HRM is likely to pick-up such abnormalities as the ports are very closely placed. HRM technique is less time consuming and easier to perform than conventional manometry.
Ambulatory esophageal pH monitoring equipment
The equipment for pH monitoring includes pH electrode, data logger and computer with software. Electrodes available for ambulatory esophageal pH monitoring include monocrystalline antimony electrodes, glass electrodes and ion-sensitive field effect transistor electrode. Glass electrodes, despite being costlier than antimony electrodes, are popular in India due to their long life. Both monopolar (requires an external cutaneous reference electrode) and combination glass electrodes (with built-in reference) are available commercially. Most laboratories, including ours, prefer combination electrode, as monopolar electrode may be inaccurate due to loose contact and changes in pH around the reference electrode due to sweating. The glass has a high electrical conductivity. Ratio of hydrogen ion concentration on the two sides of the glass is proportional to the generation of electrical potential at the liquid glass interface; measurement of pH is dependent on this potential difference. Portable solid-state data recorder store data that is converted into digital signal, transferred to the personal computer and is analyzed with software. Several commercially available software programs are available for this purpose and each has its relative merits and demerits. Technique, interpretation and indications of ambulatory esophageal pH monitoring has been reviewed recently.[25]
Technique
24-h ambulatory pH monitoring is done after overnight fast. All drugs that affect esophageal motility and LES pressure must be discontinued at least 72-h before the study. Proton pump inhibitors must be withdrawn for at least one month before the study. Procedure must be adequately explained to the patients.
Electrode calibration: pH electrode must be calibrated before and at the end of each study as failure to do so may lead to gross inaccuracy. Calibration is performed with both acidic and neutral buffer of known pH (usually pH 4 and 7).
Positioning of pH electrode: The proximal pH electrode needs to be placed 5-cm above the upper border of LES, determined by manometry. The distal pH electrode is kept in the stomach to record gastric acidity. Therefore, manometry should be done before pH monitoring. Some authors suggest positioning of pH probe by noting pH change while withdrawing the electrode from stomach, by fluoroscopy and, in reference to gastroesophageal mucosal junction noted endoscopically;[26,27] however, these methods may not be accurate.
24-h monitoring: Data logger is hanged from patient’s shoulder. He/she is asked to remain ambulatory. A diary is given to the patients with instructions to record the time of meal, symptoms and body posture. Advice to avoid acidic drinks during the study should be given to the patients. The patient should eat and drink the usual foods during the study. We do not perform pH monitoring as an outpatient procedure as we do not want to let the patients go home with the costly equipment. However, outpatient pH monitoring is more physiological than inpatient study. Once the study is completed, the electrode is removed and the signal files are downloaded and analyzed with software provided with the system.
Interpretation
The parameters that are evaluated during analysis of 24-h pH record include (a) percentage of time lower esophageal pH<4, (b) percent of reflux time in supine posture, (c) percent of reflux time in upright posture, (d) total number of reflux episodes, (e) reflux episodes of more than 5 minutes duration, (f) duration of longest reflux episode. Of these, percentage of time lower esophageal pH <4 is the most important parameter. Upper limits of normal of percentage of time lower esophageal pH <4 are 5 (total), 6 (in upright posture) and 2.5 (in supine period) in our laboratory.[25] Accordingly, gastroesophageal reflux may be erect, supine or combined. A 24-h pH record showing combined gastroesophageal reflux is shown in Figure 3 (D).
Clinical utility
Gastroesophageal reflux disease (GERD) is diagnosed by symptoms, response to proton pump inhibitors[28] and if esophagogastroduodenoscopy has already been done, by typical endoscopic findings, if present.[29,30] 24-pH monitoring is not essential in all patients with GERD. However, it is essential in patients with atypical symptoms including refluxinduced asthma; patients refractory to medical treatment and before undertaking surgery.
Combined Multichannel Intraluminal Impedance & pH Monitoring (MII-pH)
Equipment
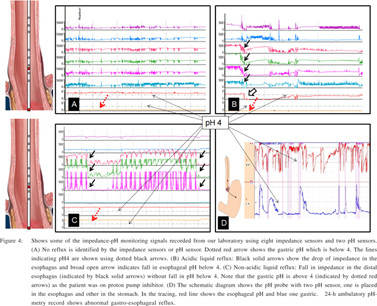
The equipment consists of impedance electrode, data logger with flash card and computer with software. We commonly use catheters with 6 impedance electrodes (impedance measuring segments) and a pair of pH electrodes (Figure 4). Electrical impedance (expressed in ohms) around the catheter in the area between the two pair of electrodes is inversely proportional to the electrical conductivity in the area between the two electrodes. [31] In the absence of swallow or reflux within the esophagus, the impedance is identified by the electrical conductivity of the inner wall of the esophagus itself and it is relatively stable, and is known as impedance baseline value. Impedance increases if gas refluxes into esophagus (belching) whereas liquid reduces it. Bolus movement recorded by impedance monitoring are either retrograde and ante-grade.[32] Retrograde bolus movements denote reflux. If refluxate is liquid, impedance drops by 50% in two consecutive or more recording sites. Antegrade bolus movement is due to swallow. The pH sensor during impedance monitoring classifies reflux episodes are categorized as acid (<4) and non acid (>4).[33]
Technique
Preparation for the test, electrode calibration and 24-hours monitoring technique are similar to the ambulatory pH-metry.
Interpretation
Parameters recorded during MII-pH monitoring include: (a) total reflux (liquid and gaseous) percent time and those in upright and recumbent posture. (b) acidic and non-acidic reflux in upright, recumbent and both posture. (c) duration of esophageal pH<4 in upright and recumbent and both the periods, (d) acid exposure percent time in upright, recumbent and both the postures, (e) mean acid clearance time, and (f) symptom correlation to reflux (acidic and non acidic).
Clinical utility
In contrast to pH-metry alone, impedance-pH metry can detect non-acid and gas reflux in addition to acidic reflux[32,33,34]. Therefore, it may be used to diagnose reflux even on treatment with acid lowering drugs.35 Impedance-pH monitoring is more sensitive to diagnose GERD. It is useful to investigate patients with atypical symptom of GERD.[36,37,38] Figure 4 shows some of the impedance-pH metry signals of patients investigated in our laboratory.
Esophageal transit scintigraphy
Scintigraphic technique using radioactive liquid or solid bolus to study the aboral and retrograde movement of the esophageal luminal contents is fairly simple to perform. It non-invasively quantifies the time, extent and pattern of the bolus clearance from the esophagus.[39] Radionuclide transit scintigraphy has many variations regarding radionuclide used, bolus content, patient position, method of image acquisition and analysis.
Technique
Patients fast overnight before the study and remain off all the drugs that can alter esophageal motility for 3-5 days. A general protocol includes image acquisition in supine position; practice swallows of bolus followed by bolus of 99mTechnitium Sulfur colloid in 10-15ml water. Dynamic images are acquired every 0.1-0.8 frame/sec by computer and gamma camera while the patient is asked to swallow. Individual and dynamic cine images are reviewed. Quantification may be performed to calculate the transit time from individual segments of the esophagus and percentage clearance of bolus. Functional condensed dynamic images give a good visual evaluation of the pattern of clearance of the bolus.
Interpretation and clinical utility
Qualitative cine images may be adequate to diagnose severe abnormalities. Some form of quantification is commonly used to diagnose less severe abnormalities and is particularly helpful in follow up of the patients after therapy. Various quantification methods have been compared. Normal mean liquid esophageal transit time varies depending on technique used and is usually within a range between 6-15 sec. Computer generated curves or functional images help in evaluating the clearance pattern. Clearance curves from the proximal, middle and distal thirds of the esophagus normally show smooth progression of the tracer activity into stomach. This pattern may be lacking in disease states. Functional images condense the dynamic image data into a single image with one spatial dimension (vertical) and one temporal dimension (horizontal). In achalasia the esophageal segmental pattern is typically flat in all the segments with little evidence of the bolus progression. Transit studies may show normal progression of the bolus through the upper and mid esophagus but prolonged retention of the activity in distal esophagus. Scleroderma patients typically demonstrate greater than 50% retention of the activity in distal esophagus even after 10 min of multiple swallows. In diffuse esophageal spasm there are multiple uncoordinated peaks representing disorganized transit of bolus through all the segments of esophagus.
Esophageal transit studies are also being used to elucidate the patho-physiological details of the disease like gastroesophageal reflux in which, contribution of delayed lower esophageal transit is hypothesized. Though manometry often scores over esophageal transit studies in diagnosis of esophageal motility disorders, transit studies may be recommended, (a) when esophageal manometry is not available or is not tolerated by the patient; (b) when manometry is equivocal or negative but reasonable suspicion of disease remains; (c) when serial changes and response to therapy need to be monitored; (d) to evaluate functional correlates of manometric abnormalities particularly for research.
References
1. Pope CE. Normal anatomy and developmental anomalies of esophagus. In: Sleisenger MH, Fordtran JS, Scharschmidt BF, Feldman M, Cello JP, editors. Gastrointestinal diseases: pathophysiology, diagnosis, management. Philadelphia: WB Saunders Company; 1993. p.311–8.
2. Dalton CB. The esophageal motility laboratory: Materials and equipment. In: Castell DO, Richter JE, Dalton CB, editors. Esophageal motility testing. New York: Elsevier; 1987. p.29–34.
3. Dalton CB. The manometric study. In: Castell DO, Richter JE, Dalton CB, editors. Esophageal motility testing. New York: Elsevier; 1987. p.36–59.
4. Vanek AW, Diamant NE. Response of human esophagus to paired swallows. Gastroenterology. 1987;92:643–50.
5. Dalton CB. Measurements and interpretation. In: Castell DO, Richter JE, Dalton CB, editors. Esophageal motility testing. New York: Elsevier; 1987.p.61–78.
6. Swift GL, Smith PM, McKirdy HC, Lowndes RH. Vector volume analysis of lower esophageal sphincter in achalasia and the effect of balloon dilation. Dis Esophagus. 2001;14:54–6.
7. Cohen S, Lipschutz W. Lower esophageal sphincter dysfunction in achalasia. Gastroenterology. 1971;61:814–20.
8. Richter JE. Normal values for esophageal manometry. In: Castell DO, Richter JE, Dalton CB, editors. Esophageal motility testing. New York: Elsevier; 1987.p.89–90.
9. Vaezi MF, Richter JE. Diagnosis and management of achalasia. American College of Gastroenterology Practice Parameter Committee. Am J Gastroenterol. 1999;94:3406–12.
10. Davies HA, Kaye MD, Rhodes J, Dart AM, Henderson AH. Diagnosis of oesophageal spasm by ergometrine provocation. Gut. 1982;23:89–97.
11. Pilhall M, Borjesson M, Rolny P, Mannheimer C. Diagnosis of nutcracker esophagus, segmental or diffuse hypertensive patterns, and clinical characteristics. Dig Dis Sci. 2002;47:1381–8.
12. Castell DO. The nutcracker esophagus and other primary esophageal motility disorders. In: Castell DO, Richter JE, Dalton CB, editors. Esophageal motility testing. New York: Elsevier; 1987.p.131–42.
13. Ghoshal UC, Kumar S, Saraswat VA, Aggarwal R, Misra A, Choudhuri G. Long-term follow-up after pneumatic dilation for achalasia cardia: Factors associated with treatment failure and recurrence. Am J Gastroenterol. 2004;99:2304–10.
14. Kahrilas PJ, Dodds WJ, Hogan WJ, Kern M, Arndorfer RC, Reece A. Esophageal peristaltic dysfunction in peptic esophagitis. Gastroenterology. 1986;91:897–904.
15. Gadenstatter M, Klingler A, Prommegger R, Hinder RA, Wetscher GJ. Laparoscopic partial posterior fundoplication provides excellent intermediate results in GERD patients with impaired esophageal peristalsis. Surgery. 1999;126:548–52.
16. Heider TR, Farrell TM, Kircher AP, Colliver CC, Koruda MJ, Behrns KE. Complete fundoplication is not associated with increased dysphagia in patients with abnormal esophageal motility. J Gastrointest Surg. 2001;5:36–41.
17. Weston S, Thumshirn M, Wiste J, Camilleri M. Clinical and upper gastrointestinal motility features in systemic sclerosis and related disorders. Am J Gastroenterol. 1998;93:1085–9.
18. Ghoshal UC, Saraswat VA, Aggarwal R, Misra A, Dhiman RK, Naik SR. Oesophageal motility and gastro-oesophageal reflux: effect of variceal eradication by endoscopic sclerotherapy. J Gastroenterol Hepatol. 1998;13:1033–8.
19. Fox M, Hebbard G, Janiak P, Brasseur JG, Ghosh S, Thumshirn M, High-resolution manometry predicts the success of oesophageal bolus transport and identifies clinically important abnormalities not detected by conventional manometry. Neurogastroenterol Motil. 2004;16:533–42.
20. Fox MR, Bredenoord AJ. Oesophageal high-resolution manometry: moving from research into clinical practice. Gut. 2008;57:405–23.
21. Bansal A, Kahrilas PJ. Has high-resolution manometry changed the approach to esophageal motility disorders? Curr Opin Gastroenterol. 2010;26:344–51.
22. Bredenoord AJ, Weusten BL, Carmagnola S, Smout AJ. Doublepeaked high-pressure zone at the esophagogastric junction in controls and in patients with a hiatal hernia: a study using highresolution manometry. Dig Dis Sci. 2004;49:1128–35.
23. Pandolfino JE, Kim H, Ghosh SK, Clarke JO, Zhang Q, Kahrilas PJ. High-resolution manometry of the EGJ: an analysis of crural diaphragm function in GERD. Am J Gastroenterol. 2007;102:1056–63.
24. Pandolfino JE, Ghosh SK, Rice J, Clarke JO, Kwiatek MA, Kahrilas PJ. Classifying esophageal motility by pressure topography characteristics: a study of 400 Patients and 75 Controls. Am J Gastroenterol. 2008;103:27–37.
25. Dhiman RK, Saraswat VA, Naik SR. Ambulatory esophageal pH monitoring: technique, interpretations, and clinical indications. Dig Dis Sci. 2002;47:241–50.
26. Mattox HE 3rd, Richter JE, Sinclair JW, Price JE, Case LD. Gastroesophageal pH step-up inaccurately locates proximal border of lower esophageal sphincter. Dig Dis Sci. 1992;37:1185–91.
27. Klauser AG, Schindlbeck NE, Muller-Lissner SA. Esophageal 24-h pH monitoring: is prior manometry necessary for correct positioning of the electrode? Am J Gastroenterol. 1990;85:1463–67.
28. Schenk BE, Kuipers EJ, Klinkenberg-Knol EC, Festen HP, Jansen EH, Tuynman AR, et al. Omeprazole as a diagnostic tool in gastroesophageal reflux disease. Am J Gastroenterol. 1997;92:1997–2000.
29. Saraswat VA, Dhiman RK, Mishra A, Naik SR. Correlation of 24-h pH pattern with clinical features and endoscopy in gastroesophageal reflux disease. Dig Dis Sci. 1994;39:199–205.
30. Armstrong D. Endoscopic evaluation of gastro-esophageal reflux disease. Yale J Biol Med. 1999;72:93–100.
31. Nguyen HN, Domingues GR, Lammert F. Technological insights: combined impedance manometry for esophageal motility testingcurrent results and further implications. World J Gastroenterol. 2006;12:6266–73.
32. Bredenoord AJ. Impedance-pH monitoring: new standard for measuring gastro-oesophageal reflux. Neurogastroenterol Motil. 2008;20:434–9.
33. Tutuian R, Castell DO. Review article: complete gastrooesophageal reflux monitoring - combined pH and impedance. Aliment Pharmacol Ther. 2006;24:27–37.
34. Tutuian R, Castell DO. Reflux monitoring: role of combined multichannel intraluminal impedance and pH. Gastrointest Endosc Clin N Am. 2005;15:361–71
35. Galmiche JP. Impedance-pH monitoring in proton pump inhibitor resistant patients: ready for clinical application? Gut. 2006;55:1379–81.
36. Tutuian R. Update in the Diagnosis of Gastroesophageal Reflux Disease. J Gastrointestin Liver Dis. 2006;15(3):243-47.
37. Bajbouj M, Becker V, Neuber M, Schmid RM, Meining A. Combined pH-metry/impedance monitoring increases the diagnostic yield in patients with atypical gastroesophageal reflux symptoms. Digestion. 2007;76:223–8.
38. Blondeau K, Tack J. Pro: Impedance testing is useful in the management of GERD. Am J Gastroenterol. 2009;104:2664–6.
39. Kazem I. A new scintigraphic technique for the study of the esophagus. Am J Roentgenol Radium Ther Nucl Med. 1972;115:681–8.